
 Vi
Vi 
What is a vitrectomy?
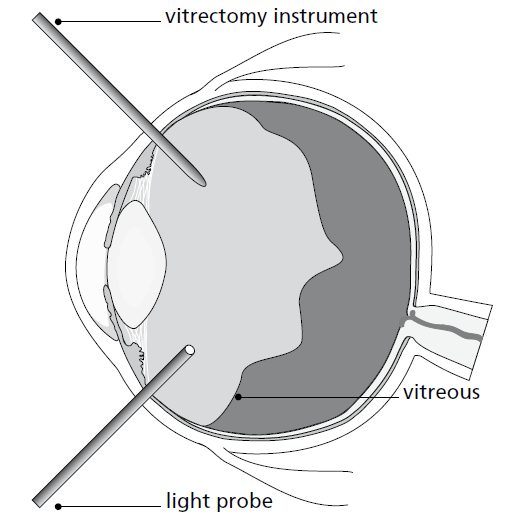
A vitrectomy is an operation to remove the vitreous humour, a clear, transparent jelly-like substance inside the eye. The vitreous lies behind the iris (the coloured part of your eye) and the lens, and is in front of the retina (back of your eye). It has no real function other than providing volume to the eye.
Why is a vitrectomy necessary?
A vitrectomy may be necessary for a number of reasons:
- Retinal detachment;
- Macular hole (a small gap that opens at the centre of the retina, in an area called the macula);
- Diabetic vitreous haemorrhage (bleeding);
- Removal of foreign body within the eye (after a trauma);
- Removal of membranes (scar tissue) from the retina, a procedure that is called membrane peel with ICG dye;
- Endophthalmitis (a serious eye infection);
- Following complicated cataract surgery where there are residual lens fragments that need retrieving, a procedure called phacofragmentation.
How is the vitreous jelly removed?
You may have your operation under a general anaesthetic (while you are asleep) or local anaesthetic (while you are awake). Your eye doctor will discuss this with you.
Your surgeon makes three very small incisions through the sclera (the white part of your eye) and using very fine instruments removes the vitreous jelly from inside.
Once the jelly is removed the retina is repaired, if necessary, foreign bodies are removed and in the case of a membrane this is peeled. In diabetic eye problems, any leaking blood vessels are sealed and retinal laser treatment is performed if required. The procedure normally takes 1-2 hours.
Does the vitreous jelly get replaced naturally?
No, the jelly does not naturally replace itself and a number of substitutes may be used at the end of the surgery. These include:
- Gas bubble, which is absorbed naturally within 2-3 weeks with a short-acting gas (SF6) and about 2 months with a long-acting gas (C3F8)
- Transparent silicone oil (which is not absorbed but is usually surgically removed at a later date)
- Air (absorbed naturally within 5-7 days).
The eye produces its own clear fluid known as aqueous humour that, as the gas or air is absorbed, will gradually fill the vitreous chamber
If there is gas bubble in your eye: you must not fly in an aircraft. The pressure in the cabin of an aircraft is dropped to about 2/3 of the atmospheric pressure. If there is gas in your eye, this will expand to 1.5 times its size, with a corresponding rise in pressure in your eye. This would be very painful and would lead to loss of sight.
It is also important to alert other medical staff if a general anaesthetic is required in the future, so that the anaesthetic teams know which gas to avoid, as the gas you may have in your eye is not compatible with the gas used during general anaesthetics. You will be given an ID wrist bracelet which will indicate the gas used and the approximate date the gas is absorbed. Please keep this ID wrist bracelet on your wrist until your doctor allow you to remove it.
What are the risks during surgery?
The procedure has a good success rate and complications are unusual. However, minor complications may occur and in most cases these are treated effectively. Very rarely complications can lead to reduced vision or loss of vision.
Other important potential risks are:
- Most patients who have vitrectomy surgery will develop a cataract (cloudiness of the lens of the eye) at an earlier age than they would otherwise. It is not possible to put a timeframe on when it might occur, however, if this happens you will require another operation to remove the cataract. Sometimes cataract surgery is performed at the same time as the vitrectomy operation;
- Infection and bleeding in the eye can occur. The risk of these occurring is very low but they are serious if they occur and can result in a permanent severe visual loss;
- Inflammation in the eye, which is treated with eye drops;
- New retinal tears, holes or detachment can sometimes happen during surgery. These can usually be treated by laser or cryotherapy (freezing treatment) during surgery;
- Raised pressure can occur in your eye. It is usually a temporary problem occurring in the first few days after surgery. In most cases this can be successfully treated with eye drops or tablets. A very small proportion of patients might need a surgical procedure to treat high pressure following surgery;
- Low pressure can also occur in the eye after surgery. Depending on the cause of the low pressure, some patients could require surgery to correct the problem;
- Failure of surgery orneed for further surgery. Vitrectomy has a good success rate for most conditions but some patients may require more than one operation;
- Very rarely after eye surgery, inflammation could develop in the other eye which can damage the vision. This is called sympathetic ophthalmia. The chance of this happening is greater if you have multiple operations on the same eye, but it is still very rare;
- Some patients may develop distortion in their vision after surgery, depending on their eye condition before surgery. This may or may not recover with time and further surgery may be required.
Your doctor will discuss these potential risks with you prior to your operation and you giving your consent.
What to expect after your vitrectomy?
The most important factor determining your rate of recovery and the final outcome is the pre-operative condition for which the vitrectomy was performed. Another important factor is your ability to comply with post-operative instructions or recommendations.
You will be prescribed a combination of eye drops to put in on your discharge home. These will help to prevent infection, reduce inflammation and rest the eye following surgery.
If gas or oil has been inserted into your eye, you will be advised to adopt your head in a certain position. This helps to ensure that the gas or oil is lying against the area of the retina which has been treated encouraging it to heal in the correct place.
What will my vision be like after the operation?
Your vision will be very blurred for a few weeks following the operation if a gas bubble is used. This is because the gas makes everything badly out-of-focus. The gas bubble will gradually get absorbed, which will appear as a wobbly black ring in your line of vision. The bubble will move as you move and gradually get smaller or break into smaller bubbles and eventually disappear.
If oil is used your vision will remain blurry whilst the oil is in your eye.
You may or may not notice a significant improvement in your vision after the operation depending on your eye condition before the surgery. Most people will notice an improvement but it may take several months before this happens.
Do I need to come back?
As the gas is naturally replaced by fluid, you need regular eye examinations at the clinic. This is to make sure that those areas of retina no longer covered by gas remain in place. The usual time intervals are after 2 weeks for the first follow-up consultation, then at another point when the gas has gone. Occasionally, the retina can get loose (detached) whilst the gas leaves the eye, or shortly after. So, any time in the next few months, if you notice a worsening in vision in between appointments, please arrange for your appointment to be brought forward.
What are the signs to look out after your operation?
- Increasing pain, redness and swelling, light sensitivity.
- Coloured discharge from your eye.
- Worsening of the vision.
If you experience any of those signs please come to the FV Hospital’s Ophthalmology Department or Accident & Emergency Department on days Ophthalmology Department is closed.









