
 Vi
Vi 
When advised to undergo a total jawbone resection to treat a large ameloblastoma, Mr C, a 34-year-old from Cambodia, was shocked and concerned about the risk of permanent facial disfigurement. Seeking an alternative approach, he turned to FV Hospital, where he was offered a conservative treatment aimed at preserving his facial appearance, with initial results proving promising.
How a Hidden Ameloblastoma Quietly Eroded the Patient’s Jawbone
In 2024, Mr C noticed a painless mass in the lower left jaw accompanied by abnormal swelling. He was diagnosed with ameloblastoma – a benign tumour that grows silently, progressively invading the jawbone. Doctors recommended a total removal of the left lower jawbone, followed by bone grafting to reconstruct the facial structure.
Fearing the permanent disfigurement from major surgery, Mr C travelled to Vietnam to seek alternative treatment options at FV Hospital.
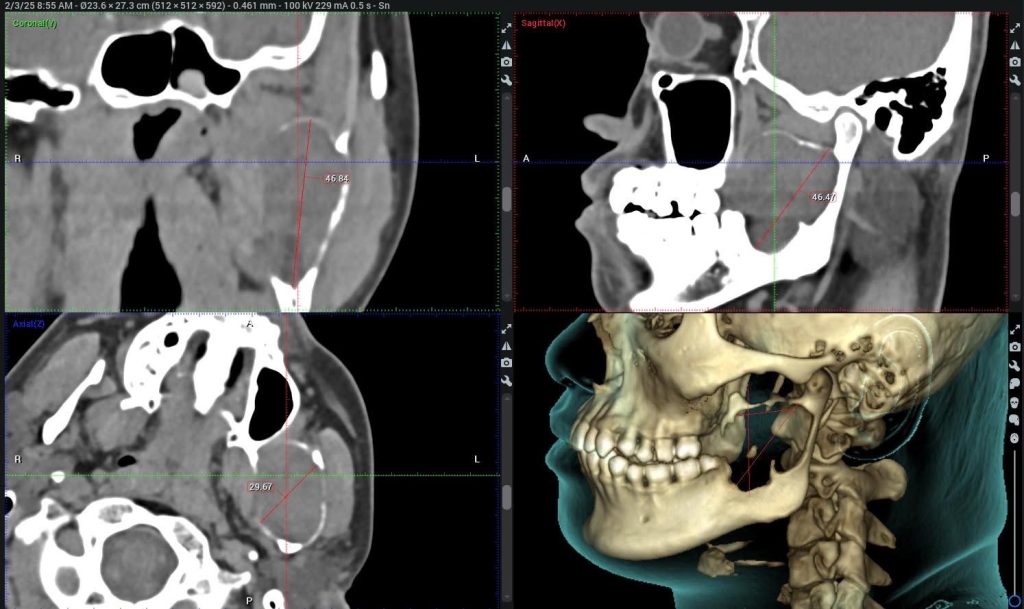
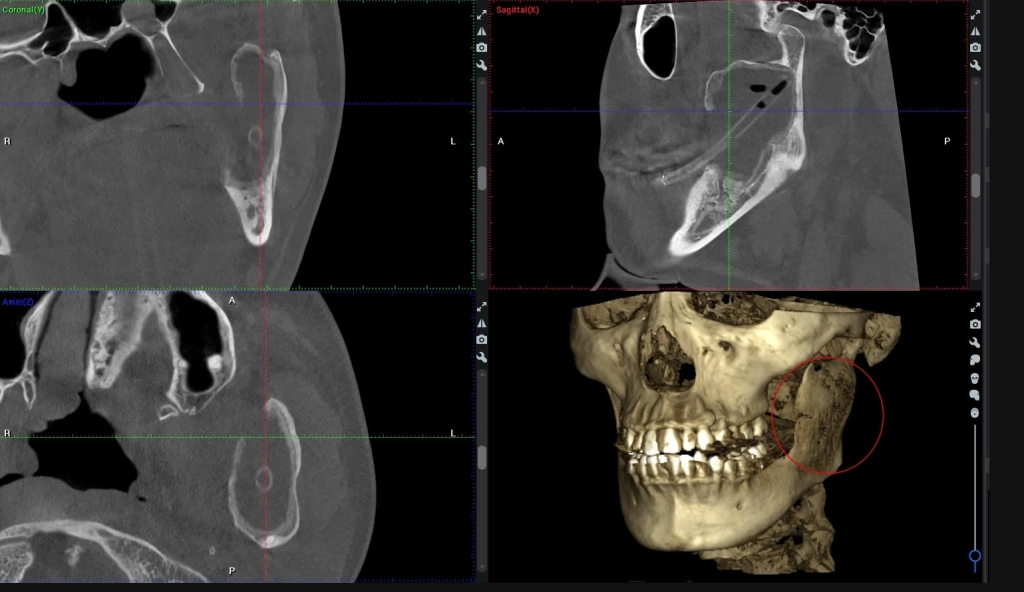
Upon examining Mr C, and reviewing CBCT (Cone Beam Computed Tomography) imaging, Nguyen Thanh Tung, MD, PhD, Head of the Oral & Maxillofacial Surgery – Dental Surgery Department at FV Hospital, identified a cystic lesion that had almost completely destroyed the lower jawbone, extending from the angle of the jaw up to the condyle. “The patient’s wisdom tooth (number 38) was impacted and fused with the tumour, which could be one of the contributing factors to the formation of the tumour,” Dr Tung explained.
Fortunately, the tumour remained confined within the bone, and the patient showed no signs of numbness in the chin or lower lip, indicating that the inferior alveolar nerve was unaffected. Despite the tumour extending into the temporomandibular joint area, the patient maintained normal mouth opening. These findings suggested that conservative treatment was a viable option for the patient.
Conservative Treatment: A Simple Approach Requiring In-depth Medical Knowledge
Had Mr C undergone traditional treatment, doctors would have performed a total resection of the left lower jawbone, followed by bone grafting to reconstruct it, using tissue from the fibula, ribs, or iliac crest. This major surgery carries a high risk of complications and can significantly impact both facial aesthetics and chewing function.
Dr Tung chose a conservative treatment approach for Mr C, using a pressure-release technique combined with cyst cavity drainage. “When the pressure within the cystic cavity is relieved, the osteoclastic cells in the surrounding bone walls cease their activity. The body then receives signals to begin the process of regenerating new bone in the walls surrounding the tumour (the tumour’s peripheral area), gradually shrinking the tumour while thickening the surrounding bone over time,” Dr Tung explained.

During the decompression surgery, Dr Tung extracted the impacted wisdom tooth (tooth number 38) and created a window into the tumour cavity through the oral mucosa. The cystic lining was sutured to the surrounding mucosa to form a permanent opening, essentially converting the cyst into a marsupialised pouch. A drainage tube was then placed to keep the window open.
A key challenge during the decompression procedure was carefully removing all tumour tissue causing internal pressure, while managing the high risk of bleeding due to the tumour’s vascular nature. Thanks to Dr Tung’s extensive surgical experience and the use of modern haemostatic tools, the surgical team was able to control the situation effectively.
After three months of treatment, the tumour had significantly reduced in size, and a new layer of bone, measuring approximately 2-3 mm had clearly formed around the cyst cavity. At his follow-up appointment in April 2025, the patient was pleased to report that he could eat and open his mouth normally, with minimal pain.
As the tumour continues to shrink and surrounding bone regenerates, Dr Tung plans a second surgery to fully remove the remaining tumour tissue while preserving the continuity of the jawbone, the nerve, and the function of the temporomandibular joint. In some cases, large cystic lesions may spontaneously regress and fully resolve following decompression.
Ameloblastoma: Risk of Overtreatment if Misdiagnosed
Ameloblastoma is a common benign tumour arising from odontogenic (tooth forming) cells, most commonly occurring in the lower jaw and primarily affecting younger individuals. Although benign, the tumour is locally aggressive, often progressing silently while gradually destroying the jawbone. This can result in facial deformity and significantly impair the patient’s ability to chew and eat.

The World Health Organization (WHO) classifies ameloblastomas into several subtypes, each with distinct characteristics and treatment approaches. Among them, unicystic ameloblastoma can often be managed using conservative methods such as decompression or simple enucleation, depending on the microscopic level of tumour invasion. In particular, intraluminal type unicystic ameloblastomas have a high success rate with conservative treatment, comparable to that of managing typical odontogenic cysts of the jaw. However, inaccurate or incomplete histopathological diagnosis, or overly aggressive surgical interventions, can result in unnecessary and severe consequences for the patient.
“If the tumour is correctly identified, particularly if it is a unicystic ameloblastoma, and conservative treatment is properly applied, we can absolutely avoid radical jaw resection for the patient, even though decompression may require several months or even up to a year,” Dr Tung emphasised.
To learn more about ameloblastoma and other oral and maxillofacial conditions, please contact Oral & Maxillofacial Surgery – Dental Surgery Department at FV Hospital or call (028) 3511 3333.











